Meet the members of our staff and discover the vision and values that drive our work.
ADA Health Policy Institute
The ADA Health Policy Institute (HPI) is a thought leader for critical policy knowledge about the U.S. dental care system.
Thought leadership for better oral care
The Health Policy Institute (HPI) conducts innovative studies on a wide range of topics on the U.S. dental economy.
HPI's Research Topics
HPI’s Economic Outlook and Emerging Issues in Dentistry tracks dentists' perspectives.
Landing page
Publications on dental care utilization and expenditures across the U.S.
Landing page
Research on dental practice modality, dentists' earnings and reimbursement trends.
Landing page
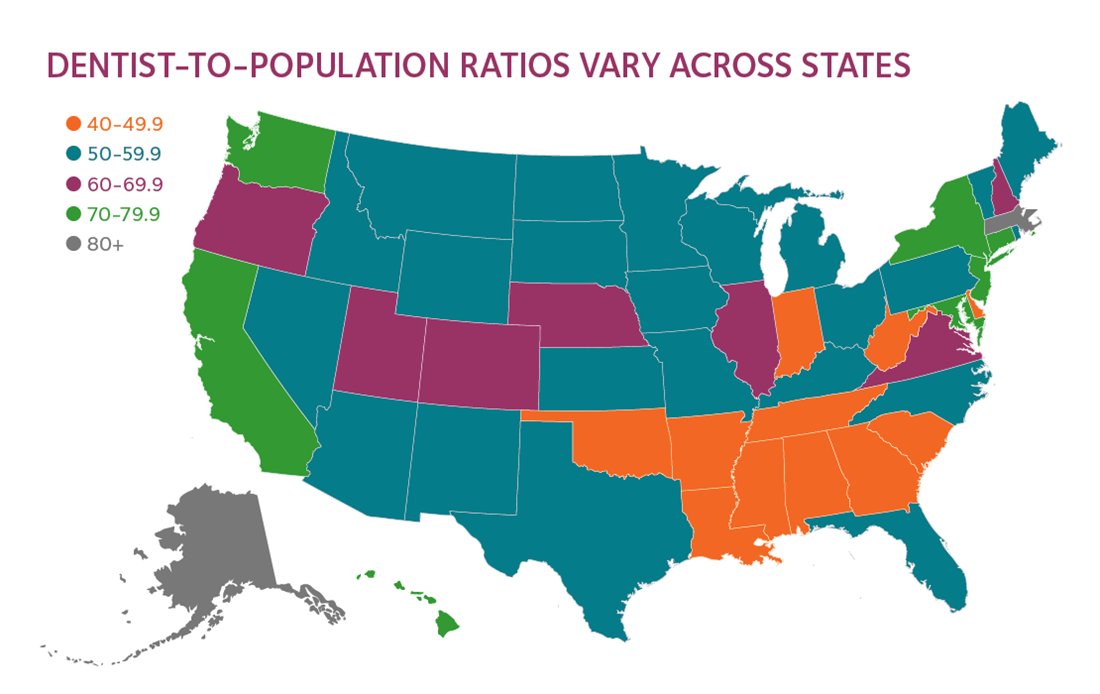
Trends in the current and future supply of dentists and Dentist Demographics Dashboard.
Landing page
Dental student demographic trends and other data on CODA-accredited dental education programs.
Landing page
Research on dental benefits, access and barriers to care, and oral health outcomes.
Landing page
HPI in the news
Browse the latest media coverage that cites HPI findings and reports.
Tools for policymakers
Crucial information for oral health policymakers and advocates.

HPI Consulting
Custom research and resources for leaders of large group practices, dental insurers, manufacturers and other decision makers.