Key Points
- The caries process is multifactorial and, over time, can culminate in localized destruction of hard dental tissues by weak acids.
- Effectively penetrating and sealing pits and fissures in the surfaces of teeth can prevent caries lesions and is part of a comprehensive caries management approach.
- Sealants are systems that can be applied to the occlusal surfaces of teeth to penetrate anatomic surface pits and fissures and form a physical barrier on the tooth surface.
- A 2016 guideline panel convened by the ADA CSA and the American Academy of Pediatric Dentistry (AAPD) developed a clinical practice guideline based on a systematic review of the literature and recommends use of pit-and-fissure sealants on the occlusal surfaces of primary and permanent molars in children and adolescents:
- sealants are effective in preventing and arresting pit-and-fissure occlusal caries lesions of primary and permanent molars in children and adolescents compared to the non-use of sealants or use of fluoride varnishes; and
- sealants can minimize the progression of noncavitated occlusal caries lesions (also referred to as initial lesions) of the tooth that received the sealant.
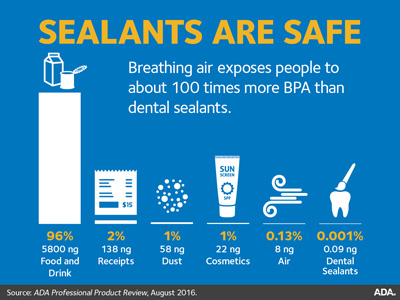
- Although dental materials used to treat and prevent caries, including dental sealants, can contribute to very low level bisphenol A (BPA) exposure for a few hours after placement, based on current evidence, there is no health concern relative to BPA exposure from any dental material.
Download Sealants are Safe for Facebook (JPG)
{kind=link}
Download Sealants are Safe for Twitter (JPG)
{kind=link}
{kind=link}
{kind=link}